
 Discussion
Discussion
Hereditary angioedema
Last updated Dec. 19, 2025, by Marisa Wexler, MS
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
Hereditary angioedema, often abbreviated HAE, is a chronic genetic disease characterized by recurrent episodes of swelling in the deeper layers of the skin or in mucus membranes. This type of angioedema has an estimated prevalence of 1 in 50,000 to 150,000 individuals worldwide.
The acute swelling attacks, which are the hallmark symptom of HAE, most commonly occur in the hands, feet, face, abdomen, and genitals, although they can affect any part of the body. In contrast to other types of angioedema, swelling in HAE is usually not accompanied by hives or an itchy rash.
HAE is caused by mutations that a person is born with, and while there is no cure for the disease, a range of treatments can be used to prevent and manage swelling.
Causes
HAE is a genetic disorder caused by mutations that are normally inherited from a person’s biological parents. In rarer cases, those mutations may arise spontaneously in someone without a family history of the disease.
There are three main types of HAE, all sharing a basic underlying mechanism, which is an overproduction of bradykinin. Bradykinin is a signaling molecule that regulates blood pressure and inflammation. It normally causes blood vessels to dilate, and renders them more permeable, or leaky, to help reduce blood pressure. However, when too much bradykinin is produced, as occurs in HAE, fluid leaks out from blood vessels and accumulates in nearby tissues, causing swelling.
HAE types 1 and 2
HAE types 1 and 2 are caused by mutations in the SERPING1 gene, which carries instructions for making a protein called C1 esterase inhibitor (C1-INH). This protein blocks the activity of two other proteins — plasma kallikrein and coagulation factor 12 — that promote the production of bradykinin. When there isn’t enough C1-INH available, bradykinin levels can rise too high and cause a swelling attack.
HAE type 1 is the most common form of the disease, accounting for about 80% to 85% of all HAE cases. In this type, mutations in the SERPING1 gene impair the production of C1-INH, causing the levels of the protein to be too low to properly regulate bradykinin production.
In HAE type 2, which accounts for most other cases of the disease, SERPING1 mutations do not affect the production of the C1-INH protein, but impair its activity and prevent it from working correctly. As a result, these patients have normal or even high levels of C1-INH, but the existing protein cannot effectively regulate bradykinin production.
HAE type 2 mutations often affect a specific part of the SERPING1 gene called exon 8.
HAE type 3
HAE type 3 is a somewhat broad term that encompasses rarer cases that are not caused by mutations in the SERPING1 gene. This form is sometimes also called HAE with normal C1-INH, because, in contrast to the more common HAE types, the levels and activity of C1-INH are both normal.
The most well-studied causes of this disease type are mutations in the F12 gene, which codes for a protein, called clotting factor XII, that starts a chain of events responsible for producing bradykinin. Mutations in F12 cause the protein to become overactive, ultimately driving the production of more bradykinin than is needed.
Mutations in other genes, including PLG, ANGPT1, KNG1, MYOF, and HS3ST6, have also been linked to HAE type 3, but these are rare and remain poorly understood. There may be additional mutations that may act as HAE causes, but have yet to be discovered.
HAE inheritance
Across all types, HAE inheritance follows an autosomal dominant pattern.
For most genes, everyone inherits two copies, one from each biological parent. While some diseases require that children inherit two faulty gene copies to develop the condition, in autosomal dominant inheritance, only one mutated copy is sufficient to cause the disease. As such, people with HAE generally have one mutated copy of the affected gene, as well as a healthy copy.
For that reason, HAE is virtually always inherited from a biological parent who has the disease. If someone with HAE has biological children, there is a 50% chance the child will inherit the mutated gene and also have the disease.
Symptoms
Acute episodes of swelling are considered the hallmark symptom of HAE. Without treatment, patients may experience bouts of swelling every 1-2 weeks, and most attacks will last for about three to four days.
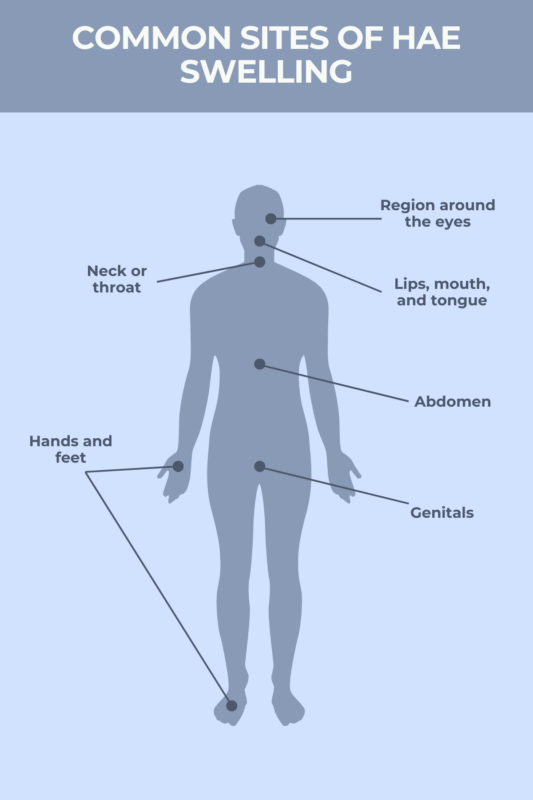
Swelling in HAE can occur in any part of the body, but most commonly affects the:
- region around the eyes
- lips, mouth, and tongue
- neck or throat
- hands and feet
- abdomen
- genitals
In addition to the visible parts of the body, swelling in HAE can occur in mucus membranes lining internal organs, including those that are part of the gastrointestinal tract. This can cause patients to experience gastrointestinal symptoms, such as vomiting, diarrhea, and abdominal pain, sometimes without any noticeable swelling.
Swelling in HAE can be uncomfortable or painful, but it usually isn’t serious. The major exception is when swelling occurs around the neck or throat, which can block the airways and make it difficult to breathe. Swelling in the throat is a medical emergency, and patients should seek immediate care as soon as they experience signs of swelling in that region.
HAE is a form of chronic angioedema, meaning patients will generally experience multiple swelling attacks over the course of their lives. This makes HAE distinct from forms of acute angioedema, where swelling usually disappears once its underlying cause is addressed.
Most patients start to experience symptoms of HAE before age 20. However, it’s pretty uncommon for swelling attacks to occur in young children. While there can be a lot of variability, swelling attacks usually become more frequent and severe in the teenage years, as patients enter and go through puberty.
Apart from swelling, some people experience other HAE symptoms, such as:
- fatigue
- headache
- unusual sensations like tingling, stinging, or numbness
- nausea and vomiting
- abdominal pain and cramping
- flu-like symptoms
Many HAE patients experience early signs and symptoms before an attack ensues. These early signs, known as prodromes, may include:
- fatigue
- joint or muscle pain
- feelings of pressure or tightness in the skin
- redness or rash
- pressure in the abdomen
- irritability, anxiety, and other mood changes
Triggers
In many cases, there isn’t an obvious trigger that leads to swelling in HAE. In many instances, swelling attacks develop spontaneously with no clear cause.
Still, some known HAE triggers may increase the likelihood of swelling attacks, including:
- exposure to certain foods and other allergens
- hormonal changes, such as fluctuations that occur during the menstrual cycle or pregnancy
- physical exertion or injury
- illness and infections
- certain medications, including some blood pressure medications and birth control pills
- surgeries and dental procedures
- emotional stress
For people living with the disease, avoiding potential triggers can be an important part of HAE management. This can include taking steps to minimize injury and prevent infection, avoiding exposure to allergens or potentially-triggering medications, and taking precautions during surgeries, dental procedures, or pregnancy.
Keeping a journal detailing events around the time of swelling attacks can also be a useful way to help identify what triggers HAE swelling.
Diagnosis
Establishing an HAE diagnosis usually begins with a physical examination after a patient experiences a swelling attack. Doctors will evaluate the type of swelling and will go over the patient’s medical history, family history, and symptoms. These initial steps can help distinguish HAE from other types of angioedema, such as acute allergic angioedema, where swelling is often accompanied by hives.
When there is no obvious cause of recurrent or chronic episodes of swelling, and all other possible angioedema causes have been ruled out, this is called idiopathic angioedema, sometimes referred to as chronic idiopathic angioedema.
If HAE is suspected, the diagnosis can usually be confirmed through blood tests that measure the levels and activity of the C1-INH protein. If a patient has abnormally low levels of C1-INH, they are typically diagnosed with HAE type 1, whereas if C1-INH levels are normal but the protein’s activity is unusually low, they may be diagnosed with HAE type 2.
Other lab tests conducted during a swelling attack may also help establish a diagnosis. For example, during HAE swelling attacks, levels of a protein called C4 are usually low, whereas those of a protein fragment called D-dimer are abnormally high.
C4 is a protein that’s part of the complement system, a part of the immune system that’s also regulated by C1-INH. In the absence of C1-INH, C4 is spent at an increased rate due to complement activation. This causes C4 levels to drop, which may be more noticeable during attacks.
Measuring the levels of another protein, called C1q, can also help distinguish HAE from acquired angioedema. This is a type of angioedema where C1-INH levels are also low, although that occurs as a result of an underlying disorder such as cancer or an autoimmune disease rather than genetic mutations. Levels of C1q are usually normal in HAE, but are low in acquired angioedema.
Genetic testing to look for disease-causing mutations can help cement a diagnosis and is the only way to definitively diagnose HAE type 3. Besides the presence of mutations in genes other than SERPING1, in patients with this rarer form of HAE, diagnosis is generally based on the presence of recurrent swelling attacks that are not accompanied by hives and in which lab tests measuring C1-INH and C4 levels are normal.
Treatment
Although there is no cure for HAE, a range of medications for HAE are available to help manage the disorder. HAE treatment can be broadly divided into two categories: on-demand treatments that are used to get swelling under control when an attack occurs, and prophylactic treatments that are routinely used to prevent and lower the risk of future swelling attacks.
Other HAE therapies are also in development, including those used orally and on-demand, and treatments using novel gene-editing technologies.
On-demand medications for hereditary angioedema
Approved on-demand treatments for HAE swelling attacks include:
- Berinert (human C1 esterase inhibitor), which is given by an into-the-vein (intravenous) injection and is approved for patients of all ages
- Ekterly (sebetralstat), which is taken as oral tablets and is approved for adults and children ages 12 and older
- Firazyr (icatibant), which is given via under-the-skin (subcutaneous) injection and is approved for adults with HAE in the U.S., and for patients 2 and older in Canada and Europe
- Kalbitor (ecallantide), which is given by a subcutaneous injection and is approved for patients 12 and older
- Ruconest (recombinant C1 esterase inhibitor), which is given by an intravenous injection and is approved for adult and adolescent patients
Most of these on-demand treatments can be administered by caregivers or self-administered with proper training. The exception is Kalbitor, which should be administered only by a medical professional.
Prophylactic medications for hereditary angioedema
Approved prophylactic therapies to reduce the risk of HAE swelling attacks include:
- Andembry (garadacimab-gxii), which is given by subcutaneous injection and is approved for patients ages 12 and older
- Cinryze (human C1 esterase inhibitor), which is given by an intravenous injection and is approved for patients 6 and older
- Dawnzera (donidalorsen), which is given by subcutaneous injection and is approved for patients ages 12 and older
- Haegarda (human C1 esterase inhibitor), which is given by a subcutaneous injection and is approved for patients 6 and older
- Orladeyo (berotralstat), a daily oral therapy approved for patients 2 and older
- Takhzyro (lanadelumab), which is given by a subcutaneous injection and is approved for patients 2 and older
All of these prophylactic therapies can be administered by caregivers or self-administered with proper training.
An oral steroid medicine called danazol has been used since the 1970s to prevent HAE attacks of all types, including those involving the skin, abdomen, and larynx (voice box). It may still be used today, especially if other treatments fail or aren’t an option, but it is generally not a first choice for prophylactic HAE treatment today.
Life expectancy
With proper care and monitoring, HAE life expectancy is generally comparable to that of the general population.
Though it can be fatal in some cases, particularly if it occurs around the throat and compromises a person’s ability to breathe, swelling in HAE is usually not life-threatening. Studies have indicated the risk of death by asphyxiation for people with HAE is relatively low, with some noting it may be higher among undiagnosed patients, emphasizing the importance of an effective diagnosis.
Living with hereditary angioedema
Living with HAE involves certain modifications that help patients minimize the risk of swelling attacks that could cause serious problems. This can include taking prophylactic medications to reduce the risk of attacks, having on-demand treatments available so that attacks can be treated promptly if and when they occur, and avoiding potential triggers.
It’s important to communicate clearly with doctors about how best to manage the disease. Patients may benefit from receiving care from a specialist who treats HAE.
Besides taking steps to manage the disease itself, people with HAE should also follow general recommendations applicable to everyone seeking to live a healthy life. Some of these recommendations include eating a well-balanced diet, practicing self-care, getting plenty of sleep, and managing stress.
It’s also recommended that patients take advantage of support groups and useful resources available to them, such as those provided by nonprofit organizations and online communities dedicated to HAE.
Angioedema News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion