
 Discussion
Discussion
Pediatric angioedema
Last updated Dec. 9, 2024, by Lindsey Shapiro, PhD
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
Angioedema, a condition characterized by swelling in the deep layers of the skin or in mucus membranes, can affect people of any age, including children.
Pediatric angioedema most often results from an allergic reaction, but it can also have other causes, including genetic mutations and autoimmune diseases, or occur as a side effect to medications. The cardinal symptom of angioedema in both children and adults is swelling, which can occur anywhere on the body, but some evidence suggests that angioedema in children is less severe than in adults.
There are various strategies for managing angioedema in children, depending on its underlying cause. Often, pediatric angioedema attacks resolve relatively quickly without serious complications, and the long-term outlook for children living with angioedema is good.
Causes
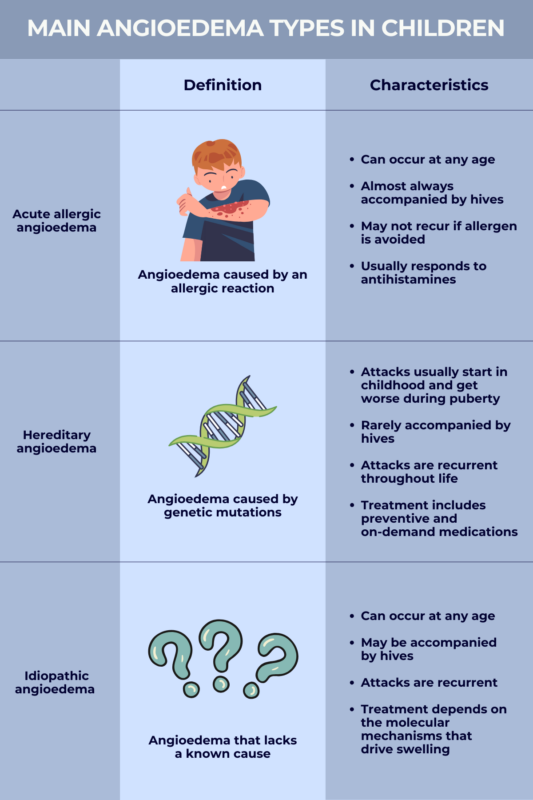
There are several types of angioedema, each with a different underlying cause. All can occur in children, though some forms are more common than others.
Acute allergic angioedema
The most common type of angioedema in children is acute allergic angioedema, where swelling occurs due to an allergic reaction. With this type of angioedema, the immune system releases an inflammatory molecule called histamine in response to an allergen (a harmless substance seen as a potential threat by the immune system), prompting swelling.
Acute allergic angioedema can result from a wide range of allergens, including foods (e.g., nuts, shellfish, or eggs), insect stings or bites, latex, certain medications, or environmental allergens. Food is a leading cause of allergic angioedema in children. Attacks usually set in quickly upon exposure to the allergen and stop once the triggering factor is identified and avoided.
Hereditary angioedema
In hereditary angioedema (HAE), genetic mutations lead to an overproduction of a molecule called bradykinin that drives swelling. HAE swelling attacks, which are recurrent throughout life, can occur at any age, but they most often begin during childhood.
Before puberty, HAE attacks in children are generally mild and infrequent, but they tend to worsen and become more common around the time of puberty. Once children reach adolescence, HAE looks similar to that in adults.
Idiopathic angioedema
About half of pediatric angioedema cases that aren’t associated with allergic reactions are idiopathic, meaning that there’s no clear identifiable cause to explain the swelling attacks.
Still, the molecular mechanisms driving the swelling in idiopathic angioedema can be determined. In some cases, swelling episodes are driven by histamine or other molecules involved in allergic reactions and have characteristics that look similar to allergic angioedema. Other cases are driven by bradykinin and will be more similar to HAE.
Acquired angioedema
Acquired angioedema is a very rare form of angioedema that’s caused by another illness, such as cancer or an autoimmune disease. This form of angioedema is not common in children, with more than 90% of cases being reported in adults older than 40.
Drug-induced nonallergic angioedema
Drug-induced nonallergic angioedema occurs as a side effect to certain medications.
In adults, this form of angioedema most commonly arises in response to angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, which are often used to treat high blood pressure. However, these medications are not frequently used in pediatric populations, so drug-induced nonallergic angioedema caused by these medications is not often seen in children.
Still, other medications that have been associated with drug-induced nonallergic angioedema in adults, such as nonsteroidal anti-inflammatory drugs, a class of over-the-counter pain medications that includes ibuprofen, have been reported to cause angioedema attacks in children.
Risk factors and triggers
In many cases, there’s no way to predict whether a child will develop angioedema, but a few factors might have an influence.
A child may be at an increased risk of an angioedema attack if they:
- had one previous attack
- have a family history of HAE
- had other types of allergic reactions to foods, medicines, insect bites, or other allergens.
Pediatric angioedema attacks may occur at random, but they can also be triggered by specific factors, such as:
- injury
- stress
- pain
- infections.
In children, viral and bacterial infections are a common triggering factor for angioedema, as they activate the immune system in ways that can drive swelling.
Symptoms
In patients of any age and regardless of the disease’s underlying cause, angioedema’s hallmark symptom is swelling, which most commonly affects the face, lips, tongue, hands, and feet, but it can occur anywhere in the body.
This swelling often manifests as large, swollen areas of skin that may be smooth or raised. It can cause the skin to become extremely tight and painful, making it difficult for a child to perform everyday activities.
In allergy-induced angioedema and cases of idiopathic angioedema driven by histamine, swelling is often accompanied by itching and hives — medically known as urticaria — which is characterized by red bumps or welts on the skin. This is not typically seen in other forms of angioedema.
For most children, the symptoms of an angioedema attack will last no more than a few days and resolve on their own without cause for major concern. However, angioedema swelling can affect the airways and cause breathing difficulties. If a child becomes dizzy or faints, experiences wheezing or voice changes, or starts to have trouble breathing, immediate medical attention should be sought.
Angioedema swelling can also affect the mucus membranes lining the gastrointestinal tract, causing a child to have digestive symptoms such as abdominal pain, nausea, vomiting, or diarrhea.
Overall, the exact pattern of swelling — and its severity — can vary a lot between children, so it’s important that parents and caregivers recognize the potential signs and triggers of angioedema in their child so that treatment, if needed, can be given as soon as possible.
Treatment
In both children and adults, angioedema treatment depends on the exact disease type that a person has. Thus, when a child comes to the clinic with signs of angioedema, a number of different doctors, including pediatricians, immunologists, allergists, and other specialists, may collaborate to establish an angioedema diagnosis, determine which disease type the child is experiencing, and then decide the best treatment approach.
Pediatric angioedema attacks often resolve on their own within a few days, especially in mild cases, and may not require treatment. Still, doctors may sometimes recommend medications to ease symptoms faster and help a child feel more comfortable.
In addition to these so-called on-demand treatments, which are used to ease active swelling attacks, pediatric angioedema treatment may also include medications to prevent swelling episodes, especially in children who are prone to future attacks, such as those with HAE.
Antihistamines
In many cases of pediatric angioedema, particularly those caused by an allergic reaction, antihistamine medications are sufficient to control both urticaria and angioedema. As their name suggests, these medications work to block the effects of histamine, the molecule responsible for driving swelling in allergic angioedema.
These medications, which are commonly used to treat allergies, can often be purchased over-the-counter and taken orally at home, but in some cases they may also be given directly into the bloodstream at a healthcare clinic.
Examples of antihistamines that can be used to treat a child with angioedema include:
- cetirizine (sold as Zyrtec and others)
- diphenhydramine (available as generics and product combinations)
- fexofenadine (sold as Allegra)
- hydroxyzine (sold as Vistaril)
- levocetirizine (sold as Xyzal)
- loratadine (sold as Claritin and others).
Because they are driven by a different mechanism, HAE and certain cases of idiopathic or acquired angioedema generally will not respond to antihistamines.
Corticosteroids and other immunosuppressants
Doctors may also prescribe corticosteroids, such as prednisolone, which have strong immune-suppressing properties, to help control swelling in a child with angioedema. Steroids are usually only taken for a short time, as they can cause significant side effects. They may be given orally, or as an injection at a healthcare clinic.
In cases where swelling is not adequately controlled with antihistamines, other immune-suppressing medications, such as omalizumab, might also be administered. These treatments can help reduce swelling and inflammation, and ease any itching that a child is experiencing.
C1-INH inhibitors
C1 esterase inhibitor (C1-INH) products are a class of injectable medications that are approved to treat and prevent HAE swelling attacks, although they can sometimes also be used for other forms of angioedema.
C1-INH is a protein that regulates bradykinin production, but most people with HAE have mutations that impair its production or function. C1-INH products are designed to provide a version of C1-INH, either lab-made or derived from human donor blood, to lower bradykinin levels and keep swelling under control.
C1-INH products that may be used as on-demand treatment for children with HAE and other forms of angioedema driven by bradykinin include:
- Berinert (human C1 esterase inhibitor), approved in the U.S. for patients of all ages
- Ruconest (recombinant C1 esterase inhibitor), approved in the U.S. for adolescents and adults.
C1-INH products that may be used as a preventive, or prophylactic, treatment in HAE children include:
- Cinryze (human C1 esterase inhibitor), approved in the U.S. for patients ages 6 and older
- Haegarda (human C1 esterase inhibitor), approved in the U.S. for patients 6 and older.
Kallikrein inhibitors
Kallikrein inhibitors work to block the activity of kallikrein, an enzyme that’s required for bradykinin production. They’re approved to treat or prevent attacks in people with HAE but, similar to C1-INH products, on-demand kallikrein inhibitors may also be used off-label for other types of bradykinin-associated angioedema.
Examples of kallikrein inhibitors that may be used in children include:
- Takhzyro (lanadelumab), an injectable preventive therapy approved for HAE children as young as age 2
- Orladeyo (berotralstat), an oral preventive therapy that can be used in HAE children who are at least 12 years old
- Kalbitor (ecallantide), an injectable on-demand therapy that can be used in children ages 12 and older.
Epinephrine and emergency interventions
If a child’s angioedema attack is affecting the airways, doctors may administer a shot of epinephrine, a hormone and brain chemical also known as adrenaline that can help tighten blood vessels and relax the airways to quickly make breathing easier. Doctors may also use other physical interventions to make sure the child can breathe properly until appropriate angioedema treatment is administered.
After an attack, a doctor might also prescribe a portable shot of epinephrine, commonly known as an EpiPen, and recommend that families always have it on hand in case a child reacts to an allergen or has another angioedema attack in the future. A doctor will also advise families on exactly when an EpiPen should be used.
Prevention
Some ways to prevent future attacks in children and adolescents with angioedema include:
- keeping substances that caused a previous angioedema attack or other type of allergic reaction out of reach
- administering prophylactic medications as prescribed by a child’s doctor
- teaching children to practice good hygiene to avoid infections, and making sure they get recommended age-appropriate vaccines
- help children avoid other triggers, such as excessive or repetitive exercise and emotional stress.
Complications and outlook
With proper treatment, most episodes of swelling in children will resolve without serious complications. However, when swelling occurs in the throat, it can cause life-threatening airway obstructions if not promptly treated.
Angioedema in children may occur as a result of an anaphylactic shock, a life-threatening allergic reaction where the immune system releases chemicals that cause blood pressure to drop and swelling to occur in the airways, leading to breathing difficulties. Parents and caregivers should take their child to see a healthcare provider right away if the child is experiencing warning signs of anaphylaxis, including dizziness and difficulty breathing. Other signs of anaphylactic shock can include flush, pale skin, and a weak or rapid pulse.
Rarely, swelling in the gastrointestinal tract can lead to serious intestinal blockages or other gut complications. If a child experiences sudden or severe abdominal pain, uncontrolled vomiting, or bloody stools, medical attention should be sought right away.
The long-term outlook for children with angioedema is overall good. Still, regular checkups with a pediatrician are important for making sure a child remains in good health and isn’t experiencing any long-term problems related to the condition.
Angioedema News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion